

CESAREAN BIRTH
We’re heading to the OR, now what?
With a few exceptions, a cesarean birth is not most people’s first choice for meeting their baby. That doesn’t mean it has to be a traumatic experience. In fact some of my cesarean moms have been the most satisfied with their births. As we’ve discussed over and over - how you were made to feel during your birth, matters much more than the individual things that happened. Is a cesarean your first choice? Probably not. But if it happens, knowing that you felt fully involved in the choices that led here, and that you were listened to and respected, will make a huge difference in working towards that fantastic birth experiences.
The rest? Knowing what to expect, and what choices are still within your grasp.

I found the quote above several years back and fell in love with it. Because it’s true.
Cesareans are not evil. They are a wonderful medical intervention that some babes need to be born safely. Knowing that your decision to choose a cesarean birth is rooted in evidence based practice and most importantly, a care team who values your experience and opinion, often helps to remove almost all of the fear surrounding these births. And knowing what to expect is the easiest way to turn your experience into a positive one if a cesarean birth becomes the best way to get your baby here safely. Demystifying the cesarean experience turns it into just another way to meet your baby. One that can still be beautiful and personalized.

Step 1: Understanding what happens during a Cesarean.
Surgery is always a bit intimidating. Let’s work to take some of the unknown out of this experience.
Step 2: Understanding why a cesarean was chosen.
Do you understand and feel confident about why this birth is moving to the OR? Even if it’s not your first choice, if you feel you were informed and involved in this decision, it’s a lot easier to feel positive about your cesarean birth.
Step 3: What choices are still available to me?
A surgical birth doesn’t mean that you have no options. Even inside the OR, you have many choices you can make regarding your birth, assuming of course that both you and baby are both still doing well.
Step 1: What To Expect During Your Cesarean

Pre Surgery Preparation
Unless this is a true emergency situation (rare), you will be brought paperwork to sign your consent. The surgeon and anesthesiologist will usually both come and explain the procedure and ask if you have any questions. If you do not already, you will have an IV placed and fluids started. You will remove all jewellery as well.
If this is a scheduled cesarean, (or even an unplanned but non emergent one) know that your time may be bumped if a more emergent situation comes into the hospital. This can feel awful, but remember it means that at this time, you and your baby are safe and healthy.

Journey to the OR and Pain Management
Once ready, you will be moved into the OR. Your support people will stay behind for now.
Inside the OR you will be moved onto the OR table. They will check your epidural and top it off if you had one, or if not, you will be given a spinal. This medication will run through the surgery so that you shouldn’t feel anything. You will lay down on the bed, but your arms should not be restrained. A catheter may be placed as well.
The sterile drapes will be set up, and the anesthesiologist will take residence near your head. They are your best friend during this birth, responsible for your well being, your pain control and any concerns you have. If you start to feel sick, anxious or feel pain during the surgery, let them know right away. It can feel claustrophobic once the drapes are set, don’t be afraid to say something if you need an adjustment.

Support Person Preparation
In the vast majority of cases, you will be able to have a support person (or two!) join you in the OR for the birth. While you are in the OR, your support person will be given a pair of scrubs to change into. They should take everything off except their underwear, socks and shoes. You will also be given a hairnet and mask. I recommend waiting until just before you go into the OR to put these on, as they can feel claustrophobic, especially when you add the stress into the mix!
Your support will then continue to wait until just before the surgery is ready to start. This can be the longest, most anxiety filled part of the day for some. Don’t worry, I’ll be there to support them. They will typically wait about 10-30 minutes, depending on the urgency of the cesarean.

Surgery Begins
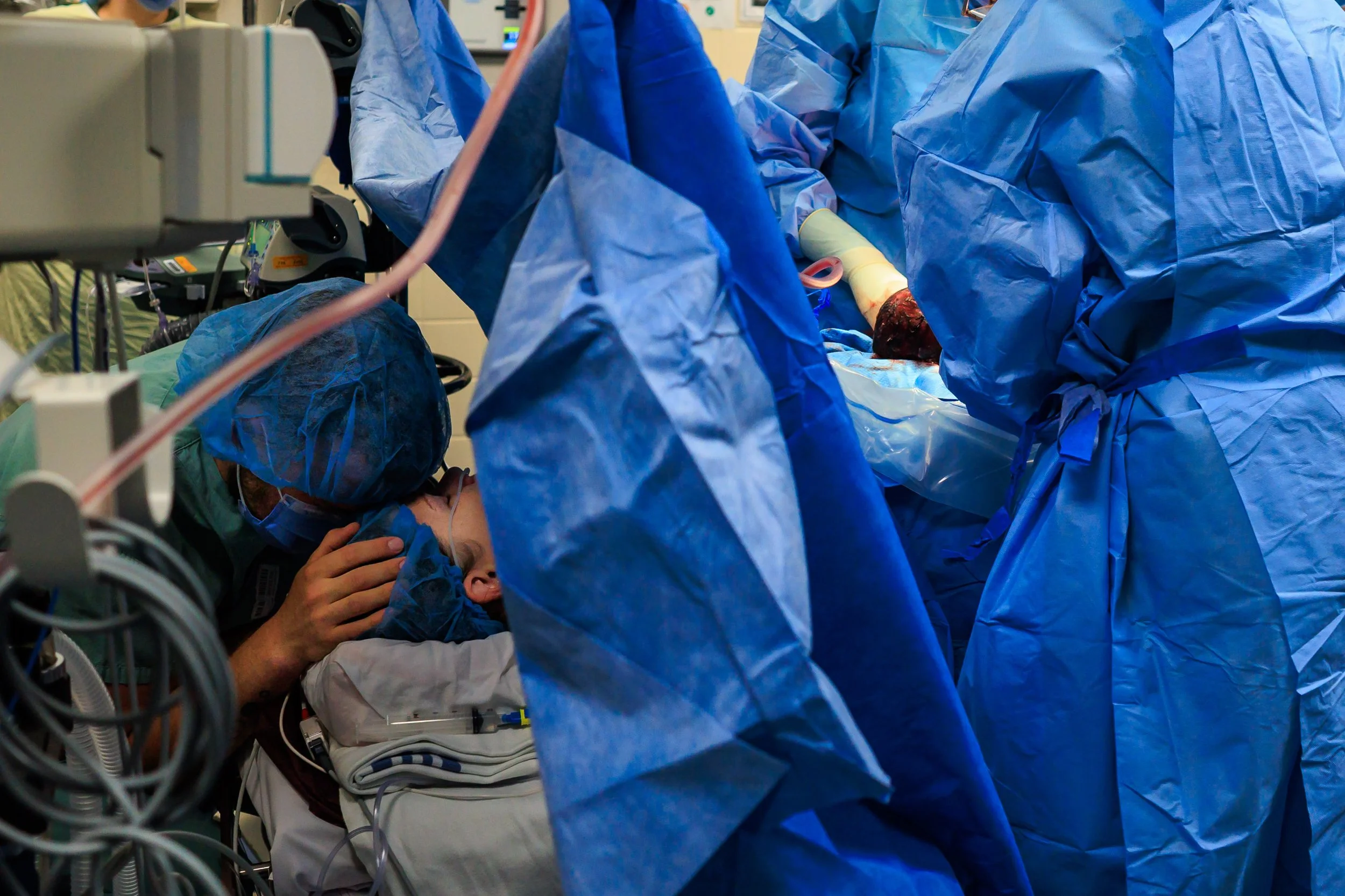
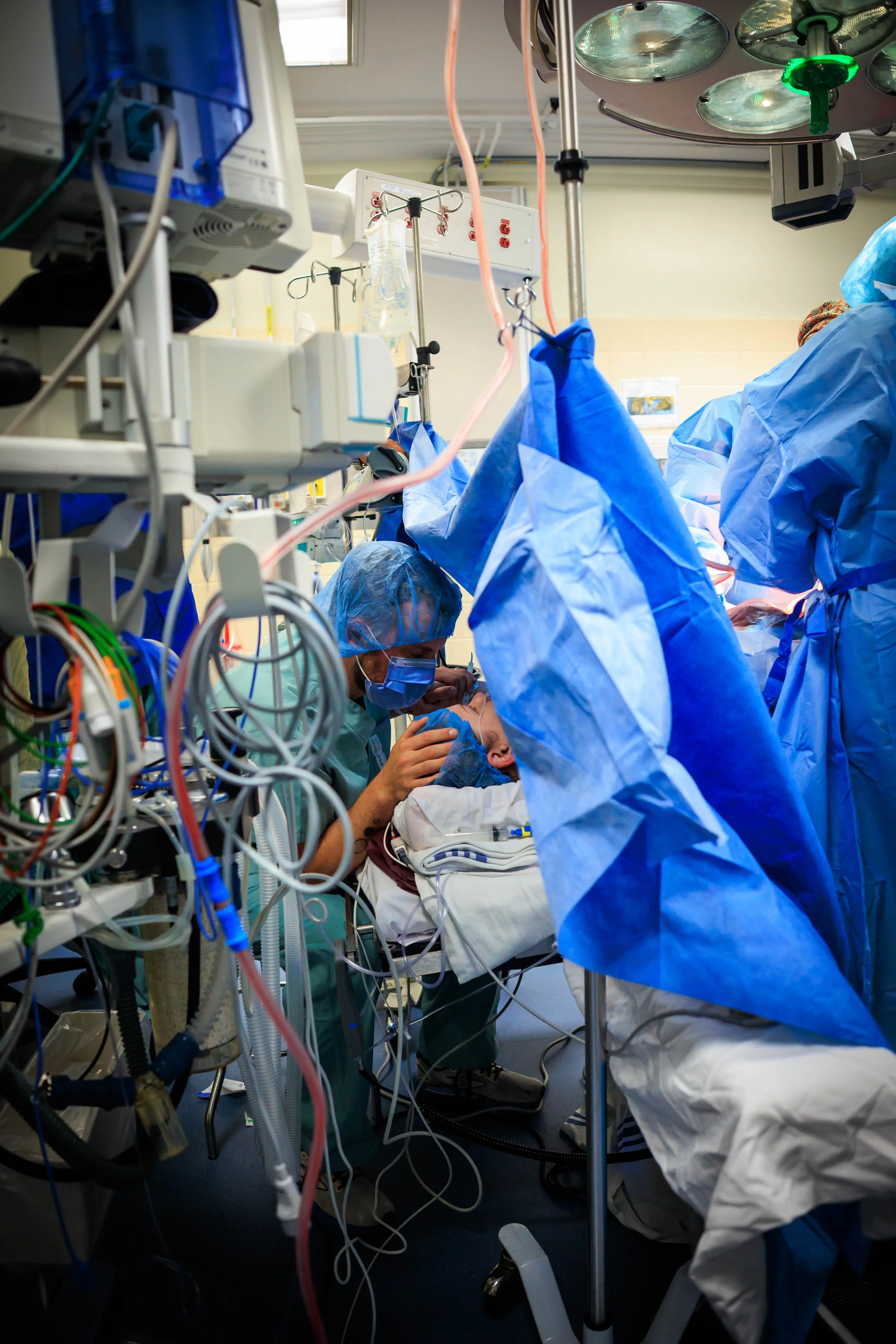
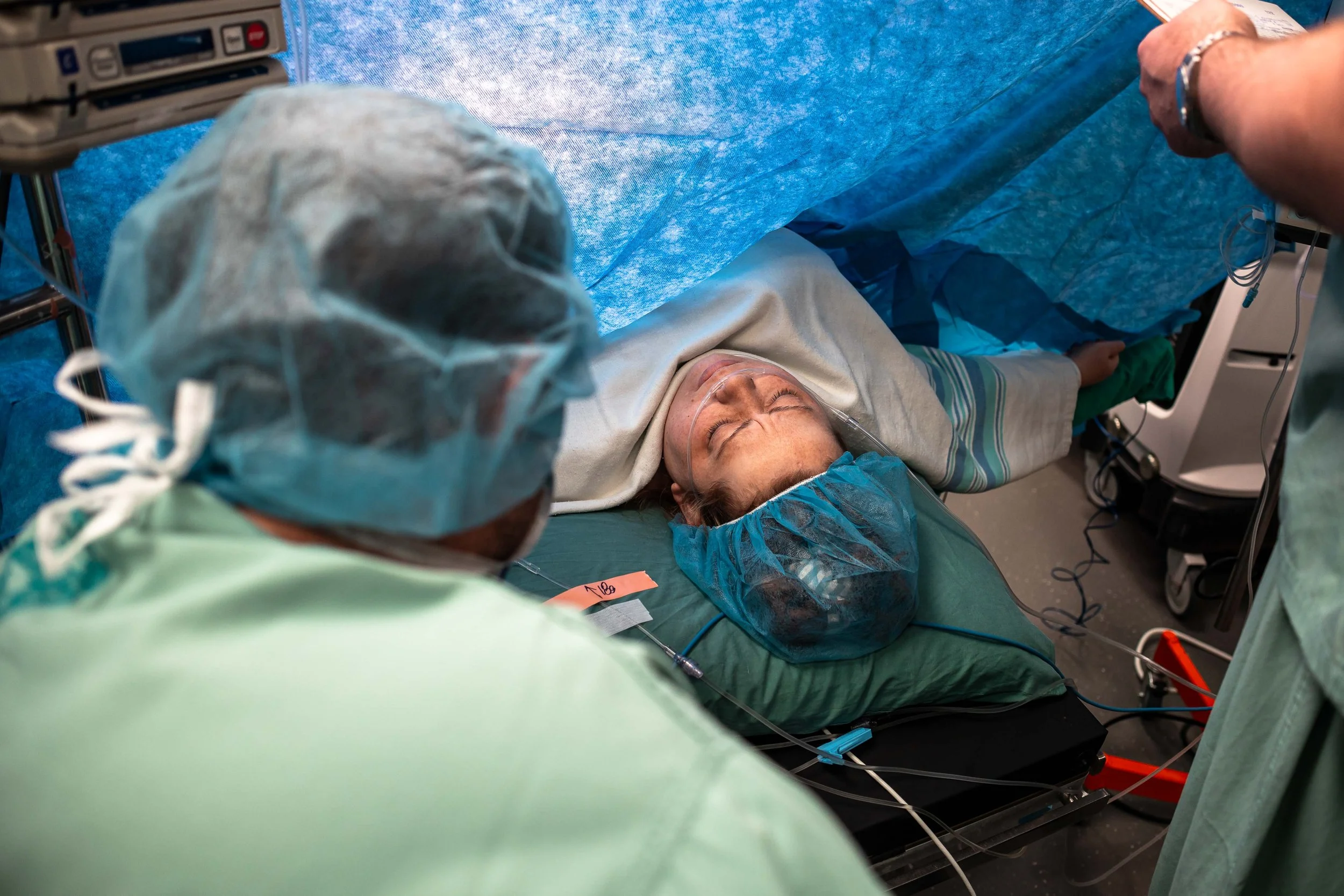
Right before your first incision is made, they will bring your support person into the room. They will be given a stool to sit on right by your head, both for comfort and fainting purposes.
Typically in the room are your OB, an assistant (often a resident), anesthesiologist, 2-4 nurses, a pediatric team of 2-3 people, as well as your support people. It can seem very busy, but everybody has a job. The photo above is a fairly typical setup. The person on the chair above your head is the anesthesiologist.


First Steps
Once everyone is settled, the first incisions will be made. Your OB will make a 4-6” horizontal incision below your bikini line, and then through the abdominal muscles. Once the uterus is exposed, they will made an incision into the lower part of the uterus.
You should not feel pain, but you may feel tugging which can lead to nausea and discomfort. You will also hear the suction working. Speak up if anything concerns you.
Support Person Jobs
If there has been a bunch of labouring before the cesarean decision, sitting down in the OR may feel like a break. But your job is far from done. The anesthesiologist will watch like a hawk for medical changes — but you are still the expert on your partner. Watch them for discomfort they may not verbalize. Speak to them and touch their head or hold their hands. All those great reassuring phrases you’ve been using? Keep it up. They’re going to need reminders that everything is normal, and that you still think they’re amazing.

The Birth
The birth normally occurs about 10 minutes into your surgery as baby is birthed slowly (usually) through the uterine incision. Your partner may be able to stand to see baby be born, and you can request to have the drape dropped a bit as well so that you can see baby better. Unless it is an emergency, most of the time a slight delayed cord clamping will be done (approx 1 minute). After this the baby is typically lifted for you to see, and then taken over to the warmer to be wiped down, and a quick vitals check.
Baby’s First Check Up
In almost all births, baby will be taken over to the warmer first for a look to ensure everything is good. They will listen to babe’s heart and lungs, do a wipe down, and then wrap and bring them back to you.
If there have been any concerns about baby (meconium, low heart rate during labour), this will be done by the NICU team, otherwise a nurse may be the one to check babe over. You can ask for your partner to join them if you’d like. Once they’ve confirmed baby is ok, they will be brought back to you to snuggle by your face.

Closure and Finishing the Surgery
The remainder of your surgery takes approx 30-45 minutes and is the time when they will deliver the placenta, repair your uterus and complete the closure of your muscle and skin. You can spend this time getting to know your baby, either skin to skin or with your partner holding babe near to you. If you wish to breastfeed, you may be able to attempt to latch or just have baby nuzzle at the breast as well, which will help once we get to recovery. It’s not uncommon to start feeling nauseous at this point, or to shiver. Communicate how you are feeling to the anesthesiologist. They can offer medications and warm blankets.

Last Steps in the OR
Once your incisions have been closed, the team will do an initial wash up of your lower half and bandage over your incision. The drape will be brought down while you are cleaned, and then you will be moved onto a postpartum gurney. At this point usually baby is placed in your arms for the journey to your recovery room.

The Recovery Room
You will typically spend approximately 2 hours in the recovery room which is located near the OR. This is so that you can continue to be monitored one on one by a nurse, and if needed, be taken back to the OR quickly.
During this time, staff will monitor both your and baby’s vitals, checking blood pressure, heartrate, your fundus, bleeding and temperature. They will also do a full head to toe newborn exam on baby. While this is typically done on a warmer bed, you can request it to be done on your bed as well! You will be offered additional pain medication at this time as your epidural starts to wear off.

Enjoy Your Baby!
Depending on how you felt during the birth, you may not have had a chance to really snuggle up and hold your baby. Recovery is a wonderful time to start fresh, say hi to baby and love up on them. If you are planning to, you can initiate breast/chest feeding at this time as well. Feeding within the first hour is associated with better feeding outcomes, but don’t worry, if you’re not up to it, we will continue working on it later!
After all exams and vitals checks are completed, you will be moved to your postpartum room with baby for the remainder of your stay. Most people stay 48 hours after a cesarean.
Step 2: Understanding the Decision for a Cesarean

Informed consent should be at the absolute forefront of every decision to move to a cesarean birth. Will you like this choice? Often not. But you should always understand the reasoning behind it, and feel you were given the opportunity to be a part of the decision. Even in an emergency, a good team will make sure you are included.
In Manitoba, about 26% of births happen via cesarean. This number can seem high and a little intimidating, but remember that this also encompasses all those cesareans that were planned ahead of time or anticipated and some of those would have been the preference of the birthing person. It also includes birthing people who plan a repeat cesarean after a previous baby was born by cesarean.
Breaking Down the Numbers a Bit…
It’s hard to find updated Manitoba specific numbers for the reasoning behind cesarean birth, but I did find a few studies looking at Canada as a whole, and honestly, I think the information can be reassuring. The primary study I reference found a Canadian cesarean rate of around 28.6% (a tad higher than Manitoba’s).
One additional study showed pre-labour or planned cesareans accounted for 15.1% of the total, while emergency or unplanned cesareans made up the other 13.5%. Meaning if you walk into your place of birth in spontaneous labour, your cesarean rate has already dropped to 13.5% (or lower, in Manitoba).
Breech birth and multiples account for approximately 4.6% of the 28% Canadian average - a whopping 63-94% of these birthers gave birth by cesarean, whether planned or not.
Those with a previous cesarean made up 9% of the 28% total cesarean rate. 80% of these births will be a repeat cesarean, whether initially planned or after attempting a VBAC (Vaginal Birth after Cesarean). For those who attempt a vaginal birth, in Manitoba approximately 28% will be successful!
In this particular study, for first births with baby head down, when labour was induced OR a cesarean planned before labour, the rate was 5% of all cesareans, or a whopping 38% for the group. However there’s a huge difference between a planned cesarean vs one that happened after an induction, and this study did not separate them. Inductions leading to cesareans is a high concern for many, as we discuss in the birth choices chapter. First though - why would someone plan a cesarean before labour if their baby is not breech, multiples or a VBAC?
Planned cesareans may occur both for the health of the birthing person, or the health of the baby. Conditions like extremely high blood pressure, placenta previa (where the placenta covers a portion of the cervix), a transverse lie (baby is sideways, not head down OR up), active infections, heart conditions in mom, fibroids, or past trauma may make a cesarean delivery safer for the birthing person. And fetal anomalies like an expected heart condition, omphalocele, anencephaly or other physical abnormalities may make a vaginal delivery risky for baby. These may also include a very small baby who may not handle labour well, or suspected very large baby.
For interest sake, I decided to finally look up my own statistics for the last few years. Over my last 56 births, 12 of those or 21% were cesareans. However 6 of those 12 occurred before labour began, either planned due to breech or other medical considerations, or due to life threatening issues like placental abruption or HELLP syndrome. One of them was even the second twin in a breech birth - Baby A was delivery vaginally, and baby B via cesarean. Looking at these completely not peer reviewed statistics - if you went into labour as a client of mine, you had a 88% chance of having a vaginal birth.
Bottom Line – For a first time birther, without high risk presentation of breech or multiples, your cesarean risk is probably closer to 15%.
What makes up that 15? Let’s take a look.

Even if you didn’t plan a cesarean during your pregnancy, we know there are still very valid reasons that may lead to a cesarean after labouring. Some of these are preventable, and some are not. We do know that inductions increase the chances of cesarean. I want to remind you that this is a GLOBAL statistic, and there are a lot of little decisions that still factor into that. I repeat - while inductions overall increase cesarean risk, this doesn’t automatically mean you’re going to end up with one. By keeping an eye on the evidence based labour practices, you can negate much of that additional risk.
Before we go too far, I want to touch on language a bit. The term ‘emergency' cesarean is used a lot. And if you end up with a cesarean after choosing to labour, it may feel like an emergency. But most cesareans, even those occurring after labouring, are not true emergent situations. We know that they are necessary, but we still have time to stop and explain what is happening, get the OR ready, and provide consent. Because of this, I cringe a bit when I hear the term emergency cesarean - We may have determined this is the new best way to get baby out. But that doesn’t mean that it needs to feel frantic and overwhelming, and that’s what the term emergency makes us think of.
In all my years as a doula, I can only remember two truly emergency cesareans. One was a ‘crash’ cesarean completed under general anesthesia after mom presented fully dilated but with extremely high blood pressure. The second situation was a placental abruption prior to labour, transported via ambulance to hospital. They thankfully were able to place a spinal, and I was able to join her in the OR shortly after baby was safely born (less than an hour after she entered the hospital).
In both these situations, the medical staff acted exactly as they should - quickly and confidently in order to keep both mom and baby safe. Other cases for truly emergent cesareans would typically be a cord prolapse (water has broken, and the umbilical cord moves past baby’s head into the vagina), extreme fetal distress that does not correct (most cases can be temporarily corrected, even if it means we make the choice for cesarean anyways), or a uterine rupture. All of these situations mean we get to the OR as soon as possible, do not pass go!
In most cases, you have more time to prepare. I typically refer to these as ‘unplanned’ cesareans, rather than emergency.

Reasons for Unplanned Cesareans
Maternal Exhaustion/ Failure to Progress - Often looped in together, this means that baby and mom are still doing ‘ok’, but we aren’t seeing the progress we need to see, and even after pain medication, it doesn’t seem in everyone’s best interests to continue to labour. This could be during labour (not dilating despite augmentation) or during pushing. This seems to be more common with inductions, and is a situation where we can take the time to weigh the pros and cons or see if there’s something else you want to try. There’s a lot of hype out there, mostly from the US, that implies cesareans are done ‘all the time’ for premature diagnosis of failure to progress. I won’t say that it doesn’t happen at all, but my experience as a doula is that this hasn’t been the case with my clients. When you go into labour informed, confident and well supported, you’re able to make decisions at each stage of your labour what your next best step is and your team works to provide options. Rarely have I seen a birthing person pushed into a cesarean during labour that didn’t seem warranted, even if just because poor mama was beyond exhausted and was ready for that option.
Maternal Health Issue - Typically this would be a prolonged period of high blood pressure, or bleeding. This indicates that while we don’t need to rush, your body isn’t handling labour as well as we’d like, and it’s probably the right move. Medications can be tried first, but if not effective, we will head to a cesarean.
Fetal Distress - This is another common reason for a cesarean choice after you are in labour. Fetal heart rate (FHR) will often change during labour (dipping during a contraction for instance) and this is normal, but usually it will recover once the contraction or push subsides. If your nurse or care provider notice that FHR does not recover after the contraction, or that it doesn’t seem to ‘notice’ the contractions at all (we call this variability), then a discussion will happen to decide if a move to the OR is appropriate. Depending on how troubling the heart rate is, may depend whether this is a slow or very quick discussion. Our concern with FHR is that it suggests that baby’s blood flow or oxygen are compromised. They’re ok with little changes, but not significant or prolonged restrictions. If the FHR has not gone SUPER high or low, usually we can try changing your medication if you’re being induced or have an epidural, change positions and up your IV fluids. Often these will resolve the heart rate issues. If not, we will switch to quickly obtaining consent and meeting baby!
Abnormal Position - Sometimes we start labouring with what we believe is a head down baby, and then determine that they’ve moved to either breech or transverse (lying sideways). In some situations, you may be able to ask about an external version to move baby into a better situation. If labour is early still, we may be able to wait and see how things progress and if baby moves from transverse to vertex. Or if baby is breech, you may choose to try a vaginal breech birth. In most cases though, these positioning problems will mean cesarean birth is necessary.
Failed Instrument Delivery - This somewhat matches up with the failure to progress above. Sometimes, even after pushing for a long time, baby just will not seem to come down low enough to be pushed out effectively. In this case, your provider may offer you a vacuum or forceps delivery, or to move immediately to the cesarean. If you try an operative delivery, they will only try a set number of times before converting to cesarean. This is to reduce stress to baby. Sometimes before attempting an operative delivery, we can try positioning changes while pushing that may help.
We are very lucky that in my experiences here within Manitoba hospitals, the decision to move to a cesarean is rarely taken lightly. Your team will discuss with you what is happening, what your options are, and why they think the right choice may be a cesarean. Remember to use your BRAIN tool to determine if you’re ready to make that choice, or if you need more information or time. In most cases, you can take a bit of time to make the right decision for yourself and baby.
Once you decide that it’s time to meet this baby via cesarean birth, you can expect to wait somewhere between 30 mins to three hours to be taken to the OR. This will be dependent on both your and baby’s current health status, availability of an OR, and availability of a team and anesthesiologist to support you. Take this time to ask questions, begin processing, take last belly photos, or even just rest! Sometimes if you’ve had an extended labour and pushing already, it can be a relief to know that you can finally relax.
Step 3: What Choices do I have for my Cesarean?

It is important to go over what your preferences may be in case of an emergency or planned cesarean birth. An unplanned caesarean can be disappointing and scary. Speaking about your preferences beforehand may help you to feel more in control of the situation and still preserve as many of your birth preferences as possible. For myself, this birth preferences sheet was longer than my vaginal birth one, because I knew my head would not be as clear if we got to this point. Here’s an edited sample of what I printed and brought with me.
Cesarean Birth Preferences
The following outlines our wishes should a caesarean birth be required. We understand that depending on the reasons for this choice, some options may not be feasible. Whenever possible, please discuss these situations with us, to help us understand the decisions.
I would like both my husband and my doula in the OR. Support during this time is crucial for me, and hiring a doula has been part of my plan to ensure a positive birth experience. If she is not allowed, I would like to speak with a patient advocate.
If baby needs to be moved from our OR to be monitored, my husband should remain with the baby at all times, and the doula remain in the OR with me.
During Surgery
• I would like to have music playing during the delivery if possible.
• We would like the option to photograph and record the baby’s birth.
• If possible, please talk me through what is happening during the surgery.
• I would like a clear drape or to be given the option to have the drape lowered to see the baby’s birth
• I would like delayed cord clamping for a few minutes and my partner to cut the cord.
• The baby should be brought to my head immediately unless medically indicated. I do not wish for baby to be wiped ‘clean’ before we meet.
• Please delay non urgent newborn procedures and exam (weight, measurements) until recovery so I can enjoy these moments too.
• Please facilitate skin to skin and early breastfeeding in the OR while the surgery is being finished.
Recovery
• My doula should be allowed in recovery with us as soon as possible if not in the birth room with us.
• I would like the catheter and IV out as soon as possible after surgery. I would prefer to have them re-inserted if needed at a later point.
• Please assist me with getting up and moving as soon as possible.
• I will be nursing on demand. Do not offer baby a pacifier or bottles. If supplementation is needed after discussing with a lactation consultant, we will offer pumped and donated milk.
Would all of these requests have been feasible? Likely not. But I went into my births knowing that if things went to a cesarean, I had laid out my preferences clearly and they wouldn’t be forgotten. Below I will list some other potential options you may have for a cesarean:
Music playing during the birth
Explanations of what is happening during the surgery
Waiting for yourself or partner to announce baby’s sex
Immediate skin to skin contact or breastfeeding
Waiting to wipe down baby - leaving vernix on
Having your doula with you
Clear drape so you can see baby’s birth
Delayed cord clamping past one minute
Maternal assisted cesarean (Yes! You can glove up and pull baby out yourself. It’s not common, but the option is there.)
Waiting to have baby’s weight done in recovery
Request for no additional talking in the OR
Warm blankets to be brought in to cover your shoulders
Request for partner to be present while placing epidural
What happens if baby needs additional care
Microbiome seeding to be done with baby
Photograph or record baby’s birth
You to be the first one to talk about baby is out
Allow baby to self deliver once incision is done
Anything else that feels important to you!



























Recovery
So you welcomed baby by cesarean birth. Hopefully it felt empowered, supported and necessary. Now what?
Even when it is 110% the right choice for your birth, recovery from a cesarean is still recovery from major surgery, and can still feel incredibly intimidating. Here’s a bit about what to expect.
Immediately after the birth, you will be given additional pain medication to take over as the epidural or spinal wears off. You may feel groggy or nauseous as well as your body adjusts post surgery. It’s not uncommon to feel itchy.
In the first few days after birth you will notice afterpains as your uterus works hard to shrink down to it’s normal size. These will be strongest on the first day, and then subside.
You will still experience Lochia - the vaginal bleeding that lasts up to six weeks postpartum. You may notice a lesser amount, but your internal wounds where the placenta detached still need to heal and your body needs to get rid of the extra blood and fluids it’s been holding onto!
Your wound will be bandaged when you leave the hospital and you will receive care instructions. By the time you go home, your dressings will likely be removed - work to keep the incision clean and dry. You may shower, but avoid baths for the first few weeks. If you have steri strip tape on the incision site, leave them alone and they will fall off when they are ready.
Keep an eye out for signs of infection, Seek care if after the first week, the wound turns angry red, is swollen or leaking fluid.
The incision will likely be tender and bruised for up to a few weeks, and will likely not feel ‘normal’ for several months. It is common for it to feel numb or a bit tingly. It is generally considered ‘healed’ after about six weeks. Do not push yourself sooner than you feel ready! Listen to your body. Gentle walking is good, but take it easy.
After your cesarean you will be restricted from lifting for a while. General recommendations are not to lift anything heavier than your baby. This includes older children and the carseat. Make sure you have someone who can help out during these weeks of healing. Remember that your muscles are still working hard to knit themselves back together.
You should avoid driving for the first few weeks, specifically until you feel fully comfortable with all turning and range of motion movements, and you feel comfortable reacting quickly (ie having to move to brake very suddenly).
Suggestions
Stool softeners can be super helpful to avoid having to strain when going to the bathroom.
If you have to cough or laugh, it’s helpful to press a pillow over your belly.
If your bedroom is on a different floor that your bathroom, it may be worth looking into setting up a temporary bed on the main floor. Walking is good, but stairs can be quite overwhelming.
Have a care plan for who is going to assist with activities like laundry, walking the dog, grocery shopping and deep cleaning.
Your incision area will likely be tender for a while - purchase some comfy dresses or loose pants to decrease the irritation.
Scar massage once fully healed is recommended by a lot of people. Look into it and see if it’s right for you.